


The T1D Exchange established a learning platform by evaluating the current state of care and engaging 10 diabetes clinics in collaborative quality improvement (QI) activities. Participating clinics are sharing data and best practices to improve care delivery for people with type 1 diabetes. This article describes the design and initial implementation of this platform, known as the T1D Exchange Quality Improvement Collaborative. This effort has laid a foundation for learning from variation in type 1 diabetes care delivery via QI methodology and has demonstrated success in improving processes through iterative testing cycles and transparent sharing of data.
Type 1 diabetes is a common, chronic illness affecting 1.25 million people in the United States (1). Fewer than one-third of people with type 1 diabetes in the United States achieve the blood glucose goals recommended by the American Diabetes Association and the International Society for Pediatric and Adolescent Diabetes (2,3), and there have been only modest improvements in this percentage during the past two decades, despite advances in pharmacology and technology (4). In a recent comparison of pediatric registries, European children were more than twice as likely as American children to meet glycemic targets (5), demonstrating that dramatic improvements in diabetes care delivery may be achievable in the United States (6).
Suboptimal glycemic control increases the risk of long-term complications such as retinopathy, nephropathy, neuropathy, and cardiovascular disease (7–9), as well as the acute risk of diabetic ketoacidosis (10). Additionally, severe hypoglycemia remains a concern for patients and their caregivers (11,12). People with type 1 diabetes are at risk for developing diabetes distress, depression, anxiety, fear of hypoglycemia, and disordered eating behaviors (13–16). Many families also experience diabetes-related conflict (17–19). These challenges are in addition to the myriad economic and social conditions diabetes care specialists and primary care providers must address as they promote the health of their patients.
Formed in 2010 through a grant from the Leona M. and Harry B. Helmsley Charitable Trust, the T1D Exchange is a nonprofit organization dedicated to accelerating therapies and improving care for individuals with type 1 diabetes. With a network of more than 80 adult and pediatric diabetes clinics serving >100,000 patients, the T1D Exchange has developed a research registry, a biobank, and an online patient community called Glu. In 2014, the T1D Exchange embarked on a mission to improve the quality of health care delivery for individuals with type 1 diabetes through the establishment of the T1D Exchange Quality Improvement Collaborative (T1DX-QI). A multicenter initiative, T1DX-QI aims to accelerate quality improvement (QI) through shared learning and continuous review of best practices and is the first learning collaborative in the United States dedicated to the care of people with type 1 diabetes (20–25). QI is the framework used to improve health care delivery and involves continuous, systematic efforts to reduce variation and improve outcomes (26).
Here, we describe the design and launch phases of T1DX-QI and provide an assessment of the QI readiness of the three adult and seven pediatric clinics that comprise the foundation of this initiative.
Research Design and Methods
Design Phase
The T1D Exchange convened a multidisciplinary leadership team to launch an idealized design process for care of people with type 1 diabetes. The goal was to catalog and reflect on current shortcomings and to generate ideas for a system-level redesign that could perform better than the current state (27). The leadership team developed a project charter to describe the project’s aim, goals, preliminary measures, and system requirements.
This phase included a series of participatory design sessions with a diverse group of >40 patients, caregivers, clinicians, and researchers. These sessions included two in-person design meetings and a series of biweekly teleconference meetings over the course of 1 year. Expertise within this group included personal experience with diabetes, clinical care, user-centered design, informatics, data management, software engineering, community integration, education, and business. Workgroups were formed to focus on different aspects of the system, including ethnography, clinical quality improvement, informatics, and community integration. The concept of coproduction was central, with patients, parents, and clinicians collaborating as equal partners to design, prototype, evaluate, and optimize the system for care improvement (28).
To describe patient and caregiver needs, the team used ethnography, a qualitative form of research that relies on in-depth observation and interviews of a group of users (29). Qualitative, semistructured interviews were completed at Cincinnati Children’s Hospital Medical Center and the University of Michigan Health System with institutional review board approval. These two centers were chosen because of their expertise in clinic design and their past relationship of working together through the James M. Anderson Center for Health Systems Excellence in the building of QI collaboratives (30). The patient diversity at these two diabetes centers was representative of the collaborative as a whole. Participants were identified to represent a variety of perspectives and included patients with type 1 diabetes (n = 12); family caregivers (n = 12); professional care team members, including physicians (n = 6), nurse educators (n = 1), social workers (n = 2), and dietitians (n = 2); health care administrators with an interest in type 1 diabetes (n = 5); and patients who were observed in clinic visits (n = 3). Interviews were recorded and transcribed, and demographic, contextual, and behavioral themes were extracted. This process allowed the design team to generate a series of in-depth personas, which are archetypes of individuals with fictionalized biographies based on the interviews. Personas were actively used to support the ideation and design work for the collaborative (31).
We conducted a comprehensive medical literature search of interventions and their efficacy on the outcomes of glycemic management and patient experience in type 1 diabetes. This search included systematic reviews, meta-analyses, and randomized controlled trials listed in the Cochrane Database of Systematic Reviews and Ovid MEDLINE. We also conducted an environmental scan of the current system to consolidate existing knowledge, including evaluations of >40 links to innovative organizations’ websites, academic manuscripts, white papers, implementation guides, and a survey of QI capacity among T1D Exchange care centers. We interviewed subject matter experts, including Dr. Soffia Gudbjornsdottir on the Swedish National Diabetes Registry, Dr. Victor Montori on minimally disruptive medicine, and Brandon Arbiter from Tidepool, an open-source secure data platform. Collectively, these resources were synthesized into a theoretical model for drivers of improved care at diabetes centers and health system levels summarized in a prior publication (32–35).
Launch Phase
The T1D Exchange surveyed candidate clinical sites for potential participation in the launch phase, gauging the interest, current QI capacity, level of involvement of patients or family members in improvement processes, and information technology landscape at each center. Seven pediatric and three adult clinics geographically distributed across the United States were selected for participation in T1DX-QI.
To build local QI capacity, T1DX-QI enrolled clinic personnel in formal training courses from the Institute for Healthcare Improvement, the QI Essentials for Managers 6-week webinar, and the Improvement Coach Professional Development Program, a course with two in-person sessions and an online component (36,37). Adapting several evidence-based tools (38–47), T1DX-QI developed a Quality Improvement Organizational Readiness Assessment (Supplementary Data), which was disseminated after QI training. This survey evaluates an organization’s foundation and culture for testing new and innovative ways to deliver care for patients with type 1 diabetes. Section 1 assesses the QI team structure, including engagement from a clinical champion and a senior department leader; inclusion of a data analyst, a site coordinator, and a patient/parent representative on the team; and the availability of an engaged and capable information technology team. Section 2 assesses the QI foundation, which includes testable change ideas, alignment with department priorities, and active monitoring of processes and outcomes, which must include patient-reported outcomes or experiences. Section 3 evaluates QI capacity by asking about proficiency in QI methodology (e.g., the Model for Improvement, lean methods, or Six Sigma methodologies), basic QI tools (e.g., process mapping, root cause analyses, and fishbone diagrams) and processes (e.g., plan-do-study-act [PDSA] cycles), and whether the site has successfully tested and scaled up more than one improvement idea. The fourth section measures QI success by asking whether teams who regularly share data with key stakeholders to improve quality have had success with relevant process (e.g., previsit planning) and clinical outcome (e.g., mean A1C, time in range, or percentage of patients with A1C >9%) measures. Each of these sections contains five components, each scored from 0 to 5. A goal was set for at least eight of 10 clinics to score >75% on the assessment by the end of the planning phase.
A coordinating center managed by T1DX-QI hosted regular meetings with six clinicians from participating clinics with expertise in QI, clinic design, and clinical informatics. This group guided teams as they began collaborating and sharing data and best practices through monthly videoconference meetings between leaders from the 10 clinics. In addition to local patient and parent involvement, a six-member parent and patient advisory board was formed to provide input on content and strategy. T1DX-QI hosted four biannual, in-person meetings attended by three to five clinicians, patient/parent representatives, and staff from each clinic. Together, these stakeholders refined quality measures, designed and executed network-wide quality improvement projects, and provided input on how data would be used and shared.
To put their training into practice and begin collaborating, leaders narrowed down the highest-priority intervention ideas identified in the design phase to three concepts that participating clinics wanted to initiate with locally adapted tests of change. These ideas were selected based on evidence from the Chronic Care Model (CCM) (48), the perception of unmet needs, available resources, motivations of participating clinics, and the potential to make rapid improvements in care delivery and patient experience. Clinics were asked to participate in at least one of these workgroups to apply QI skills gained through coursework. Six teams chose to improve depression screening processes, five teams chose to improve previsit planning processes, and five teams chose to improve processes that supported shared medical decision-making. Teams communicated via monthly Web-based conference calls and three in-person learning sessions. Through these virtual and in-person meetings, teams discussed new ideas, shared results from rapid improvement cycles, and reached alignment on measures and plans.
Using an existing online tool that supports group project management, T1DX-QI established an online collaboration space. Participants were given access, with the expectation that each clinic would share improvement cycle results monthly. The clinics were also encouraged to upload documents pertinent to ongoing project-related discussions to support seamless sharing of best practices across the collaborative.
As quality measures were prioritized, the data science team began designing a data specification document—a centralized catalog of data elements to specify the mapping from the electronic medical record (EMR) to the data files each clinic would transmit on a regular basis. This team also advised on the creation of a Health Insurance Portability and Accountability Act (HIPAA)-compliant data repository, secure encrypted transmission standards, and a Web-based portal with prototype dashboards.
Results
Design Phase
Design team participants were uniform in their acknowledgment that the state of care for people with type 1 diabetes needs radical transformation, and the project charter summarized a consensus approach. Discussions sparked by invited experts, the medical literature search, and the environmental scan all supported the concepts that the current system is unreliable, fails to meet patient and family needs, costs too much, generates evidence and knowledge too slowly, and lacks methods to translate findings rapidly into practice.
The ethnography exercise revealed common themes for patients and families affected by type 1 diabetes, including that there are no “vacations” from the disease, that it is more productive to focus on developing care routines than to allow yourself to place emotional value on glycemic outcomes, that diabetes has consequences for everyone in the family, and that care team members’ efficacy is challenged by time constraints, poor continuity, and burnout. The ethnographic personas for people with type 1 diabetes are summarized in Figure 1. The full ethnography report is available online (49).

Summarized ethnographies for people with type 1 diabetes. CGM, continuous glucose monitoring; pump, insulin pump.
Summarized ethnographies for people with type 1 diabetes. CGM, continuous glucose monitoring; pump, insulin pump.
The design team generated a diverse list of 84 intervention ideas. These concepts acknowledged the spectrum of capabilities across centers to participate in QI, the U.S. health care system’s increasing affinity for value-based payment models, an increasing emphasis on patient-centered outcomes research, the opportunity to align clinic goals with consensus guidelines, and the need to leverage available technology to minimize the burden of data collection while facilitating care delivery and QI projects. Using an impact effort matrix, a common QI tool, we narrowed the list of potential interventions by ranking them along two dimensions: perceived impact on outcomes and degree of knowledge on how to implement. Each of the high-priority interventions was explored using the personas generated through ethnography to explore how a proposed intervention could affect a variety of users of the type 1 diabetes health care system. The result was a prioritized, robust set of ideas with potential for having a breakthrough impact on health, care delivery, and research for people with type 1 diabetes.
A key driver diagram was then developed to organize these interventions and map necessary key changes and how each would address the collaborative’s aims (Figure 2).

Launch Phase
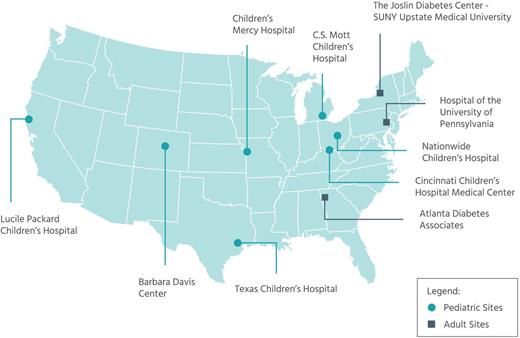
Clinics participating in the T1DX-QI launch phase are shown in Figure 3. Collectively, they serve >24,000 patients with type 1 diabetes.
One of the first steps to spark improvement after clinics were selected for participation was to enroll their clinical champions and support staff in formal QI coursework. Immediately after the training, 60% of clinics met the goal of 75% on the QI Organizational Readiness Assessment that was set by T1DX-QI to build a foundation for transformational change. Six months later, as clinic personnel had begun engaging in collaboration among diabetes centers, the proportion of clinics meeting that goal was 80%.
One of the high-priority interventions was integration of psychosocial screening into medical care. The depression screening workgroup shared resources and designed PDSA cycles to develop and refine processes, adopting interventions around the following themes: 1) consistent screening and referral criteria, 2) integration into workflow, 3) acceptance from families and staff, 4) adequate social work and psychology referral resources, and 5) incorporation of health information technology. Based on the heterogeneity of resources and experiences at participating sites, a goal screening rate of 80% was selected to reflect both realistic and aspirational goals across the collaborative. Screening increased from 10 to 67% of eligible patients across clinics over 18 months. Figure 4 shows a run chart displaying performance on this goal over time. Two clinics achieved their own goal of screening >90% of eligible patients during this interval. Additional clinics continue to join the screening intervention with reliability across the network continuing to increase over time.

Depression screening run chart. Monthly aggregate percentages of patients with type 1 diabetes screened for depression at seven T1DX-QI sites from April 2016 to July 2018.
Depression screening run chart. Monthly aggregate percentages of patients with type 1 diabetes screened for depression at seven T1DX-QI sites from April 2016 to July 2018.
Two other high-priority interventions were previsit planning and shared decision-making. Previsit planning elements included asking patients/families about their needs and self-management goals; ensuring that all patients have documentation with a standardized diagnosis code in the EMR; reviewing and scheduling appropriate screening tests; and ensuring that medication refills are completed. At baseline, three of five clinics in the previsit planning workgroup did no previsit planning, and the process was not systematic in the other two. Previsit planning workgroups shared experiences and developed consensus on which information was best to gather for upcoming visits (with emphasis on patient needs), tested and adopted methods to gather information and to communicate patient needs effectively, and developed processes to monitor planning rates across clinics. For previsit patient needs, clinics improved collection of information from 5 to 96%, with the largest gains experienced by a clinic that incorporated electronic tablets to document patient responses.
The shared medical decision-making workgroup was composed of care team members and patients who worked together to improve health care delivery and patient experiences. Teams proposed solutions and identified high-value outcomes for patients and providers and tested those ideas with PDSA cycles. The workgroup selected meaningful measures to chart progress; teams reported improved discussions and increased uptake of continuous glucose monitoring.
Throughout this phase, data collection for key process and outcome measurements was done by clinic personnel and manually uploaded to the coordinating center monthly. Clinics reported data in aggregate but did not upload detailed patient-level or encounter-level data. Across T1DX-QI, best practices, document templates, and other ideas were stored and shared in a common online platform.
Data specification for the collaborative has two parts: a core section, defining data that apply to patients in any health care setting, and a diabetes-specific section, defining data specific to patients with diabetes. By the end of the planning phase, the two clinics spearheading this effort had successfully mapped data from two different EMR systems, Epic (Epic Systems Corporation, Verona, WI) and Cerner (Cerner Corporation, North Kansas City, MO), and had begun transmitting data monthly to a new, secure, HIPAA-compliant database hosted by the T1D Exchange.
Discussion
The T1D Exchange has engaged 10 diabetes centers from the T1D Exchange Clinic Registry Network caring for children, adolescents, and adults with type 1 diabetes in building a learning collaborative that is improving care delivery and outcomes for people with type 1 diabetes. A spectrum of stakeholders methodically identified critical gaps in the current care delivery system and prioritized interventions. QI training increased local expertise, and targeted initiatives solidified those new skills by putting them into practice. A sharing community was cultivated through regular calls, in-person learning sessions, and transparent data-sharing.
Many of the high-priority interventions our group identified are grounded in the CCM (50), including previsit planning, population management, psychosocial supports, and shared decision-making. Others reflect infrastructure needs for a young QI network, including a data registry, a common online collaboration space, and ongoing, formal QI methodology training to support QI capacity at each clinic. Although much of this work focuses on the role of endocrinologists’ offices, stakeholders recognize the importance of collaborating with primary care providers to improve communication and coordination of care. One specific area of opportunity is improved information flow for items such as psychological screening results, mental health referrals, ophthalmologic exams, and laboratory tests. Moreover, primary care providers and diabetes specialists are partners in addressing their mutual patients’ social determinants of health.
Over the past 25 years, numerous diabetes registries have been created throughout the world (51). Some are primarily research-based and focus on describing network-wide outcomes (52,53), whereas others also perform benchmarking to allow comparisons among clinics (54–57). National and international benchmarking has been associated with improved A1C trends, although it is unclear what specific practices have driven these improvements (55,57). Relative to the United States, European A1C trends in type 1 diabetes pediatric populations are lower and have decreased substantially in the past 25 years, but data are not available for similar comparisons of A1C trends in adults. Some potential contributing factors to these differences may be better health care access, less complicated payer systems, higher physician- and staff-to-patient ratios, and informal sharing of best practices among centers. We are not aware of any other networks in the United States or internationally that are dedicated in part or in whole to type 1 diabetes and that provide the robust infrastructure of a learning collaborative.
Numerous active learning networks serving people with chronic diseases have demonstrated improvements in patient outcomes (58). Collaboratives reporting success have generally addressed relatively straightforward aspects of care, had a strong evidence base, and focused on a clear evidence-practice gap in an accepted clinical pathway or guideline (59). Notable successes in collaboratives with structures similar to ours are reductions in adverse drug events, central line–associated blood stream infections, and catheter-associated urinary tract infections by Children’s Hospitals’ Solutions for Patient Safety (60); improved growth parameters in infants born with single ventricles in the National Pediatric Cardiology Quality Improvement Collaborative (61); and increased rates of children with Crohn’s disease and ulcerative colitis who are in remission in the Improve Care Now network (20).
Uniting patients and their families alongside clinicians, researchers, and QI experts in this continuous learning format facilitates shared understanding and iterative system redesign, leading to more reliable, proactive care (62). With these elements now in place, our next phase will prioritize improving glycemic management for patients who are at high risk for poor outcomes. To accomplish this, clinics will continue to share diabetes education materials and identify variations in processes and outcomes. The depression screening workgroup will continue, while a new workgroup will reduce the number of patients who are lost to follow-up, as care improvements are unlikely to benefit patients who are disconnected from the clinic.
Strengths of our approach include the initiation of improvement projects early in the launch phase. This helped clinic leaders gain executive and operational support. Additionally, nascent teams learned quickly from their more experienced colleagues through the sharing of template documents, best practices, and general QI expertise. With the collaborative as a forum for frequent interaction, centers rapidly improved care processes, including incorporation of depression screening into clinical practice as recommended by the American Diabetes Association’s Standards of Medical Care in Diabetes (13).
At the institutional level, varying interpretations of patient privacy laws and human subjects protections have, in some instances, resulted in slow progress. We addressed this challenge by limiting the use of patient identifiers to only those absolutely necessary and building a secure, HIPAA-compliant data infrastructure. With strong support for increased sharing and transparency from members and local executive sponsors, T1DX-QI is committed to preventing competitive comparisons that would threaten the cooperative culture.
Comparing metrics other than A1C has been challenging because many clinics have independently developed their own unique fields to record items of interest for people with diabetes. For example, it has been difficult to interpret variation in the very important outcome of severe hypoglycemia event rate because sites collect data at different time points (emergency room visits vs. self-report at office visits) and use slightly different definitions, input parameters (numeric vs. text), recording methods (patient filling out a survey vs. health care team asking structured questions during the office visit), and look-back periods (since the last visit vs. in the past year). Therefore, normalization to a common standard is a difficult but crucial step. For some items, this process simply involves mapping structured data to the correct items, whereas for others, such as the situation with severe hypoglycemia, clinics have had to make integrated changes to data collection methods and field parameters as well.
Because the process of mapping EMRs to data files for uploading was not complete by the end of the launch phase, in these phases, we relied on manual data extraction and manipulation at each site to report summary data to a central database. This process is time-consuming, error-prone, and unsustainable. For these reasons, in the next phase of T1DX-QI, a central data infrastructure with agile, self-service reporting will give clinics a comprehensive, uniform view of their data, allowing us to identify and understand variation across the collaborative.
Data accessibility is a common and difficult barrier to QI work in health care (63). When we first tried to compare data among centers, there was a wide spectrum of abilities among clinics to access and work with their own EMR data. Some clinics had internal databases and dedicated reporting personnel who could quickly respond to data requests, whereas others were frustrated by months-long wait times to run even simple queries. Several institutions allow clinic personnel to run self-service reports within the EMR to pull all encounters or patients within a department, whereas other institutions either entirely deny clinic personnel access to reporting tools or restrict reporting to only the patients of a single provider. We addressed these challenges by providing users with data use cases, generating opportunities for clinical teams to advocate for better data access. Some clinics were able to train personnel to access clinical data and prepare it for uploading. Also, by patiently working with local information technology leadership, teams were able to get local leadership to prioritize most of the critical data requests.
Similarly, clinics began this initiative with variable readiness to engage in QI work. With formal QI training and early engagement in collaborative work, leaders emerged, and expertise rapidly developed. With several team members engaged in QI at each center, participating groups are able to execute single-center projects and work toward the common goals of the collaborative to improve A1C trends for patients at high risk for poor outcomes.
As T1DX-QI grows, this collaborative will improve care for people with type 1 diabetes across the United States. Clinics within the collaborative will benefit from Web-based and in-person meetings at which stakeholders will evaluate variation among clinics and share best practices. Clinics not able to participate in T1DX-QI may still benefit from the knowledge shared in future publications about successful interventions tested within the collaborative. As T1DX-QI demonstrates improvements, clinical champions within and beyond our collaborative will be able to point to these examples as justification for increased data quality and access to facilitate QI in their own clinics.
Conclusion
Major gaps persist between the needs and expectations of people living with type 1 diabetes and their current experiences of care. T1DX-QI brought together 10 leading diabetes centers serving a large number of patients with type 1 diabetes in the United States for the first time and demonstrated early success in designing and implementing processes through cooperative sharing of methods and data. In the next phase, clinics will focus improvement work on patients at high risk for poor outcomes by continuing to increase and maintain rates of depression screening, increasing the number of patients who check their blood glucose at least four times per day or use continuous glucose monitoring, and reducing the number of patients who are lost to follow-up.
Article Information
Acknowledgments
The authors acknowledge the faculty, staff, and people affected by type 1 diabetes at each center for their valuable contributions. Additional thanks go to John Chaffins for work on the diabetes ethnography report.
Funding
The Helmsley Charitable Trust funded this work.
Duality of Interest
No potential conflicts of interest relevant to this article were reported.
Author Contributions
G.T.A. wrote the manuscript. All other authors reviewed/edited the manuscript. G.T.A. is the guarantor of this work and, as such, had full access to all the data and takes responsibility for the integrity and accuracy of the information reported.
This article contains supplementary materials online at https://clinical.diabetesjournals.org/lookup/suppl/doi:10.2337/cd19-0032/-/DC1.